Your gifts helped build an innovative research space that is pushing the bounds of laboratory design and scientific collaboration
It took leadership and a few design risks, but pediatric cancer researchers in Calgary now have a modern, open-concept collaborative research space to call home — thanks to you.
The new laboratory space provides the perfect environment for researchers, grad students and postdoctoral scholars to investigate the biology of childhood cancer and blood disorders.
Challenging how we think about lab design: modifiable workspace
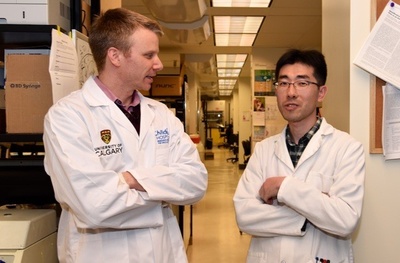
Guided by her vision for a transformative lab, Dr. Jennifer Chan, the Kids Cancer Care Chair in Pediatric Cancer Research, worked with IBI Group Calgary and the University of Calgary Facilities team of architects and planners to push boundaries and challenge traditional notions of laboratory design.
One of the many work spaces in the new lab
The result is an open-concept lab with shared workspaces equipped with fully configurable benches, specialized research rooms, student workspaces accessible through sliding glass doors and glass-walled supervisor offices along the outer edges to create an unbroken sight line across the facility.
“Our new space is very different than any other on campus,” says Chan. “The lab design allows for easy reconfiguration to accommodate future technology or new equipment — it’s like Lego. That’s the beauty of it. We’re working as we intended in a modifiable space. Although complete future-proofing is a challenge, we can still anticipate that change will happen.”
Jane Ferrabee, the U of C architect, and the U of C Facilities team that designed and built the space pushed themselves to think about their standards more critically to provide a space that allows researchers to work more efficiently and collaboratively.
“We saw this as an opportunity to explore innovation and go to new places in lab design,” says Ferrabee. “It challenged everyone involved — from electrical, IT and lighting to the lock shop and furniture — to think differently about the way we do things.”
Lab design fosters environment for improved teaching and learning
With the new research facility, Chan saw an opportunity to create an improved team environment, to cultivate new ways of teaching and learning in the lab and to strengthen the connection between medicine and basic science.
“We’re changing the culture of how we work — any time there’s a change, there’s an opportunity to improve the work culture,” says Chan. “We’re promoting the culture of the group with our decisions.”
The Power Plant is a part of the Collaborarium, a lunch room and place of collaboration.
Chan explains how the new lab set-up fosters collaboration: With the old lab space, it was like “sitting at a bar, facing forward with your food in front of you — you’re in your own compartment. This new approach is like a dinner setting, where everyone is facing each other with food in the middle, and everyone is communicating and collaborating around the table. We took our then-current notion of open concept and looped it into a circle.”
With private spaces on the outer edge, common spaces in the middle and sliding glass doors connecting everything together, students can get their work done in the quiet workspaces, while still keeping an eye on what’s happening in the lab. This spatial layering means students are close to their group, their work and their supervisors’ offices, allowing for close-knit interactions and mentorship between student and supervisor. The set-up also facilitates passive supervision, which is important for safety and productivity.
“It builds a sense of community,” says Chan. “You see someone working and it inspires and motivates you to work.”
The new research space was made possible by generous donations from you through the Alberta Children’s Hospital Foundation, Kids Cancer Care Foundation of Alberta and the Alberta Cancer Foundation.
— Revised with permission from the University of Calgary
Luke Simpson, getting ready to shave his lid for a kid
LEAD Technologies Inc. V1.01
BBQ grillers ready to go
A little off the top
Looking good Dwayne
Here we go!
For the first time in Canadian history, more than 30 pediatric cancer research and funding groups have joined forces through the Terry Fox PROFYLE initiative, a pan-Canadian project that will give young people with high-risk cancers a fighting chance.
Short for PRecision Oncology For Young People and spearheaded by the Terry Fox Research Institute (TFRI) in Vancouver, PROFYLE is providing $16.4 million to date to establish molecular profiles of patients’ tumours, which have resisted conventional therapies, in order to identify potential new avenues for treatment.
Thanks to your support, Kids Cancer Care is a partner in this national research effort that is pooling resources and bringing together research and clinical expertise to give kids with no more treatment options hope.
PROFYLE was developed with kids like Joel Zukowski in mind. Joel was 10 years old when he was diagnosed with medulloblastoma, a type of brain cancer. He relapsed at the age of 15 and exhausted all treatment options. Sadly, Joel passed away in October 2015 at the age of 16, after a long courageous battle with the disease.
One of the hardest days in Ed Zukowski’s life was telling his 16-year-old son there was no hope left in his battle with cancer. “It’s one of the most difficult discussions I had with Joel, figuring out how to tell him there was no more hope. He didn’t give up. He kept trying. That’s why research is important. You can’t give up.”
“We think about the day Joel was first diagnosed,” says his mother Dale Zukowski. “What if there was no understanding of chemotherapy, or radiation or surgery. If they didn’t do research, Joel may not have made it more than six months after being diagnosed.”
Project lead Dr. David Malkin, based at The Hospital for Sick Children (SickKids) in Toronto, says PROFYLE is bringing together the entire pediatric and young adult national clinical and research expertise to offer precision medicine in a way that has never before been offered in Canada.
University of Calgary clinician-researchers Dr. Victor Lewis and Dr. Jennifer Chan will co-lead the research project in Calgary. Lewis will help identify and treat patients, who may benefit from being enrolled in PROFYLE. Chan will ensure the collection of and access to the right kind of tissue and fluid samples for research into treatment options. The nationwide bio-specimen collection protocols are being developed by Chan, as is the associated clinical data repository, which will be facilitated by the Clinical Research Unit at the Cumming School of Medicine.
Dr. Jennifer Chan gives Joel’s mother Dale Zukowski a tour of her lab at the University of Calgary, which is home to the national bio-bank for PROFYLE.
“We now know brain cancers in adults are not the same cancers that develop in children,” says Chan, who holds the Kids Cancer Care Chair in Pediatric Oncology Research. “We’ve learned that while the tumours may appear the same to the naked eye, and even under the microscope, at the molecular level, they are very different, and that means we need to develop new treatment protocols for kids.”
“We are thrilled to see the Terry Fox PROFYLE initiative come to life,” says Christine McIver, Founder and Chief Executive Officer of Kids Cancer Care. “If we are going to make any progress in treating incurable children’s cancers, we need collaboration at all levels of society – government, industry, universities, hospitals, charitable organizations, individual and corporate philanthropists. PROFYLE is that collaboration and will bring hope to Canadian families who currently have no hope for a cure. We’re so grateful to our generous community for making this possible.”
“It’s generous support from the community that makes innovations and advancements for kids possible,” says Saifa Koonar, President and CEO, Alberta Children’s Hospital Foundation. “Working alongside partners like Terry Fox PROFYLE and Kids Cancer Care helps us keep kids’ health a research priority.”
While there has been dramatic improvement in treatments and outcomes for many pediatric cancers over the last three decades, for the 20 per cent of young people whose cancers continue to spread, return, or resist treatment, outcomes remain grim.
“Maybe in 20 years a child with the same cancer as our Joel-Bear survives. I wish that was my kid, but Joel lived six years longer than a kid 20 years ago and we’re very grateful for that,” says Joel’s mom.
Thank you for bringing hope to children by supporting research.
Victor Lewis, MD is an associate professor in the departments of Oncology and Pediatrics at the Cumming School of Medicine and a member of the Alberta Children’s Hospital Research Institute and the Arnie Charbonneau Cancer Institute.
With your support, Calgary researchers are investigating an aggressive brain cancer with the hope of slowing – and one day stopping – its fatal progression.
Last year, Lyndsay and Kevin Heaton faced the unimaginable. After a year of aggressive cancer treatments, their daughter Jessica passed away just after her first birthday. Losing Jessica is devastating for the Heaton family, but they are confident her short life will have purpose. When asked if they would consider donating her tumour to medical research, the Heatons knew exactly what that purpose was – to advance glioblastoma research for children like Jessica.
Dr. Marco Gallo is investigating epigenetics and epigenomics of brain tumours, with a special emphasis on glioblastoma (GBM)
With your support, the Childhood Cancer Research Program has recruited a bright new cancer researcher to Calgary. Dr. Marco Gallo recently joined the Experimental and Applied Therapeutics research effort at the University of Calgary and Alberta Children’s Hospital Research Institute, where he is investigating the epigenetics and epigenomics of brain tumours, with a special emphasis on glioblastoma (GBM).
GBM is a highly aggressive cancer that begins in the brain and almost always recurs after treatment. Most GBM patients do not live longer than a year after diagnosis and fewer than five per cent are alive after five years.
Dr. Gallo is hoping to change this.
Studying the DNA structure of GBM cells, Dr. Gallo and his research team have discovered that GBM stem cells have a characteristic way of packaging their DNA. Armed with this knowledge, Dr. Gallo hopes to develop targeted drugs, capable of altering this DNA packaging to minimize, and one day prevent, the chances of relapse.
While their ultimate goal is to eradicate GBM altogether, their immediate goal is to turn GBM into a chronic illness – something that is no longer life-threatening but requires life-long management.
First, they must learn how to keep the cancer from growing and spreading. To do this, Dr. Gallo and his team are studying GBM samples from U of C’s Tumour Bank. Generously donated by families who have lost loved ones to glioblastoma, these tumour samples are vital to Dr. Gallo’s work. They are accelerating the progress of finding a cure.
“We are so grateful for the families who have made the very emotional decision to donate tumours to support our research,” says Dr. Gallo. “We take this responsibility very seriously and we are determined to reduce the number of families who face this diagnosis and provide more options and more hope for the ones who do.”
The Heaton family are hopeful that Jessica’s tumour will help shed light on GBM, so other families won’t have to lose their children to this cancer
Knowing that researchers are working to help families like their own gives Lyndsay and Kevin hope. “Their fight is our fight and through Jessica and the wonderful researchers who work with her legacy, we’re able to have hope that someday other families won’t have to experience the loss of their children,” says Lyndsay. “This work very much helps keep our hope alive and underscores for us that Jessica’s life was so incredibly special and meaningful.”
Thank you for keeping hope alive
Adapted with permission from the Alberta Children’s Hospital Foundation.
Dr. Doug Mahoney’s lab is one of three in the world looking at a new immunotherapy combination that is showing promise for killing cancer.
Immunotherapy is a promising new arena in the global fight against cancer, where scientists and clinicians search for ways to harness the body’s own immune system to attack and kill cancer. Thanks to your support, a Calgary research team has made an important discovery in immunotherapy that uses existing drugs in a whole new way.
Dr. Doug Mahoney
“What we found is a combination of cancer therapies that complement each other to help the immune system clear the cancer,” says Dr. Doug Mahoney, a Kids Cancer Care-funded researcher at the University of Calgary’s Cumming School of Medicine and the Alberta Children’s Hospital Research Institute. “Our results suggest that we’ve been looking at these cancer drugs the wrong way — as tumour-targeting drugs — instead of what we now feel is their most important biological role: as immune stimulating therapy.”
Ramping up the immune system to kill cancer
Cancer cells are able to survive because they know how to hide from the body’s immune system. They also know how to control certain immune cells. Some cancerous tumours can reprogram immune cells to block other immune cells from attacking, leaving the tumour free to grow.
Treatments aimed at revving up the immune system’s attack on the cancer may be the most promising approach to cancer therapy since the evolution of combination chemotherapy. Research shows that single therapies, targeting only one part of the immune system, are effective in treating only a small percentage of patients. Results from Dr. Mahoney’s research are consistent with other recent findings, which suggest that smart combinations of therapies are even more effective in battling some cancers.
L-R Doug Mahoney with Dae-Sun Kim, the study’s lead author
A two-pronged approach
In Dr. Mahoney’s study, researchers combined two therapies, each targeting a different part of the immune system. The first one boosts the immune system, followed by a second one, which stops the tumour from reprogramming immune cells.
“This combination of drugs allowed the immune cells to do what they’re supposed to do,” says Dr. Mahoney. “We were able to cure cancer in 20 to 60 per cent of our animal models. It’s a very promising result against two very deadly forms of cancer: an aggressive breast cancer and a rare pediatric muscle cancer.”
When the researchers added a third complementary immunotherapy, the cure rate went as high as 80 to 100 per cent. Results of the study are published in Nature Communications.
Drugs seen in a new light
“These results change a lot,” says Dr. Mahoney. “What’s interesting is that neither drug was developed as an immunotherapy. For nearly two decades they have been studied for their ability to directly kill cancer cells. Viewing these drugs through the lens of immunotherapy, will impact the way we study them and try to figure out how to make them work better. From a clinical perspective, it changes the way we will try to translate these drugs.”
Mahoney says we’ll know more about the impact this study will have on cancer patients in the next five years. His lab is one of three in the world looking at this immunotherapy combination. In the other two locations, clinical trials are about to start based on a similar results.
~ Revised with permission from the University of Calgary’s Cumming School of Medicine
Years ago, when I was a small child, I received a new cancer treatment that saved my life. Right now here in Alberta there are children who need new treatments because current therapies are not working. To show you how important these treatments are I’d like to share my story.
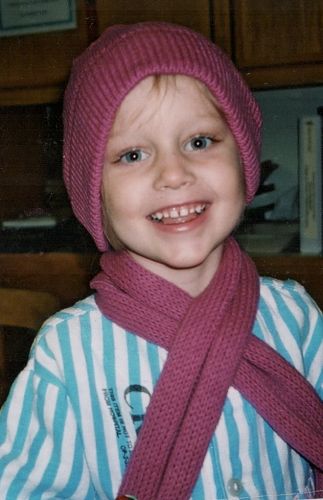
Kate’s cancer journey began when she was four
It starts way back in September of 2001 when I was four and my Mom and Dad noticed that I was unusually crabby and irritable. I wasn’t myself at all. Normally I was a happy and energetic kid. But, at that time, I was so tired I used to curl up on the couch and have a nap after breakfast. Sometimes, climbing the stairs was just too much. I would wait at the bottom of the stairs for my mom or dad to carry me up to my room. My parents thought my change in behavior was due to the recent changes in our life. I had just begun pre-school and my mom had just started working again.
Eventually, my skin became so pale and my eyes, so puffy, that my parents took me to the doctor. In the beginning, the doctors thought my symptoms were from allergies. Then I started having these high fevers, so we took a trip to the emergency, where they finally did blood work.
Although my family wanted answers, no one was prepared for the shocking news and the terrifying statistics that came with the results of my blood work.
At first it looked good. Doctors originally thought I had acute lymphoblastic leukemia (A-L-L), a leukemia with high survival rates in children. But when I went in for a test the next day to confirm the diagnosis, the doctors hit us with even worse news. With sinking hearts, my Mom and Dad learned that I didn’t have A-L-L. I had a cancer that was very aggressive and not often found in children. Acute myeloid leukemia. My long-term survival rate was suddenly cut in half.
Knowing that 25% of children with A-M-L don’t survive the first phase of chemo, the doctors offered my parents a new treatment protocol. I was one of the first patients at the Alberta Children’s Hospital to ever receive this treatment.
And so I began my first of four rounds of chemotherapy. Strangely, instead of making me sick, at first, the chemo made me feel better. My body wasn’t producing red blood cells or platelets and I had just received my first of many, life-saving blood transfusions. I was coming back to life again.
I finished the first half of that round of chemo and had a three-day break. I looked better than I had in months and we were excited to get our family pictures done.
But by the ninth day of treatment, I had zero white blood cells and the fevers began. They were relentless, hovering between 38 and 41. The drugs that once made me feel better were now making me sick. When I finished that first round of chemotherapy, they put me on the strongest antibiotics possible. Without any white blood cells, my body had nothing to fight infection on its own. Even the strongest antibiotics didn’t work.
Those hours you spend with or without white blood cells can make all the difference. It can determine whether or not you live. But the antibiotics can only do so much without help from your body. It was critical to get my white blood cells back up…so I began daily injections. After 48 hours in ICU, new blood work brought some good news. My white blood cells were coming back and, after a bone marrow biopsy, they discovered I was in remission!
That was round one.
Due to the complications I experienced during the first round of chemo, the doctors changed my second round. Despite the changes, the second round hit me hard. My weight dropped dangerously low. I wasn’t eating and I had excruciating pain in my chest. When the pain in my chest grew, they did some tests and found I had fluid around my heart and scar tissue in my lungs. I was four years old and I had suffered a heart attack! They did a laparoscopic lung biopsy to remove the fluid around my heart. But it wouldn’t budge. Finally they used a much larger needle and extracted the fluid.
After the chest tube was removed, I finally took a turn for the better. I wanted to eat for the first time in months. When I found out that Santa was coming to the hospital, I got super excited. And, for the first time since I’d gone into the hospital, my mom believed I would be home for Christmas.
She was right. I got a two-hour pass to go home on Christmas Eve. Although I spent most of the evening in my father’s arms, it was amazing to finally be out of the hospital.
I began my third round of chemo in the New Year and then my fourth. During my fourth round of chemo, I had a fever for 28 days! I ended up with another fungal infection in my lungs. By the end of the last round of chemo and, after 7 months in the hospital, my parents couldn’t believe they were finally taking me home.
Last day of chemo and ready to go home
Mom tells me that the shock of hearing the words, “Your child has cancer,” cannot be explained. The fear and uncertainty ran so deep, she felt like her world had stopped.
How does a child survive cancer? How do you take care of such a sick child and still care for your children at home? How do manage to go to work each day, when you’ve been sleeping on a cot next to your daughter’s hospital bed?
My bothers and I became my mom and dad’s total focus. Their daily routines were filled up with us, constantly spelling each other off for work or hospital shifts. My mom had only been back to work for three months when I was diagnosed. Needless to say she quit her job and I became her new daytime focus. My brothers were in school, so my mom would get them off to school in the morning and then come to the hospital to relieve my dad who spent every night with me — either on a cot or in a Lazy Boy. My dad would head to work for a few hours and then pick up my brothers from school and have dinner with them. Then around seven o’clock, my dad would come back to the hospital, relieve my mom, who spent every day with me.
They did this for seven months! They had very little time together and carried around an enormous amount of stress and anxiety.
My brothers Owen and Evan were only six and seven and they were feeling really lost during this time. With only one parent around at any given time and a sister in the hospital, they were forced to grow up too quickly. They had to answer questions that no child should have to answer. Questions about cancer, chemo, hair loss, even worse, death.
That’s where Kids Cancer Care came in. They scooped us off that summer and gave us the magic of camp! They connected us with kids who knew exactly what we were feeling. They gave us a place where no one stares and where no one has to answer questions or feel like they need to hide.
After that week at camp, we started feeling like kids again and, my parents had time to regroup. It was then that they realized we were going to be alright. We were all okay. Finally.
Kate at the 2012 High Hopes Challenge
But really it wasn’t until Christmas 2002, more than a year after my cancer diagnoses, that the cancer-focus of our family finally started settling into the background — not our of our minds completely, but moving to the sidelines.
My mom says sometimes she doesn’t know how we all survived it. But somehow we did. She says you find the strength and courage you need and you learn that you have inner reserves you never knew you had.
Seeing me go through this was terrifying for my parents. The intense schedule they had to keep was physically demanding and emotionally exhausting. Cancer is tough on kids but sometimes I think it’s harder on the parents.
I wouldn’t be here today if not for that new treatment protocol. It was tough on my body, but it saved me. That treatment would not have been possible without research. It seems almost miraculous when I think about it.
I hope you realize now why I am so grateful for people who support Kids Cancer Care’s research program. Thank you. Please remember that the research you are supporting today could save a child’s life.
~ Kate
Kate’s photo gallery
Kate at Parents’ Quest
Mason’s journey began in December of 2013 when a large lump appeared on the right side of his neck. I will never forget how my stomach dropped when I saw this mass. It instantly scared me. I contacted my husband Diego at work, right away he could hear the fear in my voice so he dropped everything and we rushed Mason to the Children’s Hospital. They did a few tests, concluded it was simply an enlarged lymph node and sent us home with antibiotics. The next day, the hospital called with test results telling us he had strep throat, so they changed his antibiotics to something stronger. We thought this was a little odd as he had no strep throat symptoms, but we followed the doctor’s instructions.
Mason with his family.
The pharmacy had only half of the antibiotics we needed, so four days later we went back to pick up the rest. The pharmacist saw Mason’s lump, and alarmed at the mass, she first asked, “Is that what the antibiotics are for?” We nodded yes and she asked if it had gotten smaller. We responded, “No, it is getting a little bigger.” She directed us back to the hospital, because the antibiotics should have started to decrease the lump by then.
Back at emergency, we were told to finish the antibiotics as some take longer than others to take effect. We went home growing more and more anxious. That evening, Mason spiked a high fever and spent the night getting sick. In the morning, the lump was even bigger. We went back to the hospital for a third time that week wanting answers. Something was obviously wrong.
The medical staff at the hospital were stumped. All of Mason’s tests were coming back normal and he was feeling fine. We were referred to an ear, nose and throat specialist who eased our worry by telling us it was not the big bad ‘C’, but simply a swollen lymph node full of clear fluid. Because it was just before Christmas break, it was decided to re-evaluate the lump in the New Year. As we were putting our jackets on to leave, the doctor called us back into the room, offering to give us some peace of mind over the holidays. He offered to prove the lump was just clear fluid by putting a needle in the lump and extracting what was in the lump. So, four of us held Mason down. The needle went into his neck, and again but the doctor could not extract a thing. The room instantly went cold and tense. The doctor quietly walked me back to reception and gave us his fist appointment after the holiday break, while Diego snuggled with Mason, trying to calm him down.
Mason and Mom
Christmas was cautious. I know that may sound funny; we all tried hard to make the best of the holidays, but in the back of our minds we were terrified. That lump continued to grow and, as parents, you simply fear the worst.
January 8th, 2014 we met with the ear, nose and throat specialist again. He took one look at Mason’s neck and said it had to be taken out ASAP.
Two days later, on the 10th of January, Mason had the lump removed in day surgery, a procedure that felt like it took forever. At 2:41 pm we were asked to come into a little office where we were told they had performed a freeze screen test in the operating room and confirmed it was lymphoma cancer.
Mason was six that day in January. Telling a six-year-old he has cancer, what cancer is and what could possibly happen to him was an out of body experience for me. He’s six. How is this possible? He is only six. Our world spiraled out of control. The next eight hours were filled with meeting the oncology team, answering a lot of questions, hearing a lot of information I could not possibly understand and a lot of disbelief.
We were able to go home for a couple of days after that first surgery and before being admitted to the oncology unit. Mason had a lot of questions; we did our best to answer them. But mostly, we snuggled, cried and did our best to prepare for the battle ahead.
The next week, all the tests necessary to determine his complete diagnosis were done: bone marrow, CT scans, ultrasounds, X-rays, countless blood tests and a lymph node biopsy from a slightly larger node on the other side of his neck.
We finally received his complete diagnosis on Wednesday, January 16th. Mason had stage 4 Burkitt’s lymphoma. He tested positive for Burkitt’s on both sides of his neck and 5 per cent in his bone marrow. Of course, we jumped on the computer and googled Burkitt’s. Pictures for Burkitt’s are shocking. Researching what our son had and what the treatment might entail kept us up all night. We cried harder and longer that night than any other time; not our son, not our six-year-old baby.
The next morning brought a new determination; there were no options in this journey. We had to win. And with that determination, Team Mason was born. Our family of four, our extended family and our incredible friends all became part of that team.
One of many days spent at the hospital.
Mason went through five rounds of extremely intense chemotherapy. Each round brought on different challenges, but Mason never ever quit. He didn’t want to do it for one more second, but he never quit. He was aMazing. He is the bravest person I know.
The Alberta Children’s Hospital is such an amazing place. Not a place any family wants to know well, but we are so lucky to have it here in Calgary. We met many incredible people on unit one: doctors, nurses, families, volunteers and organizations. Being on that unit was humbling to say the least. It really grounded us and made us realize how fortunate we really were. When we first arrived, we thought our world was crashing down; however, when we found out Mason’s complete diagnosis and treatment plan, we were certain Mason was going to beat his cancer. We met so many other families who did not know their future. I can not possibly imagine their fear and pain.
We spent 60 nights at the hospital in unit one. It became our home away from home.
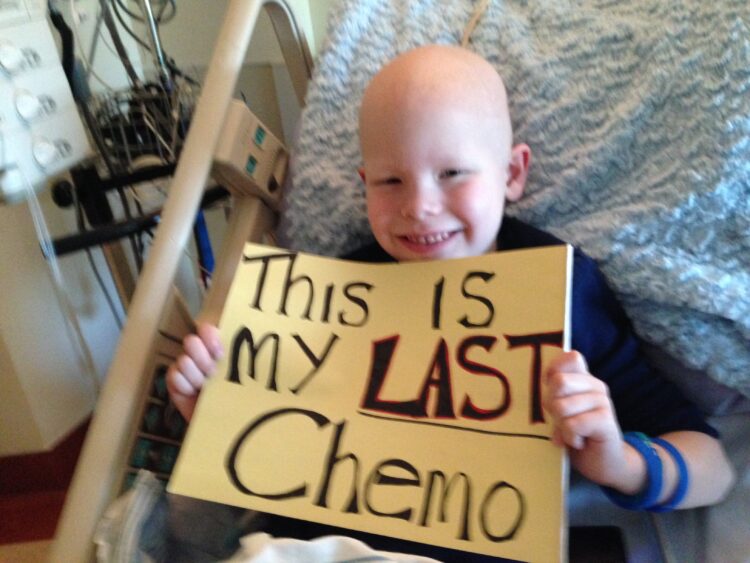
On May 14th, we heard the magical words every oncology family dreams of hearing: “Mason is in remission.” He then went through his last round of chemo, like a champ. He strolled into that unit, said “Hi” to all the ladies in the nurses’ station, walked into his room and started to set up his bed and room the way he likes it. Through that week, he showed everyone his magic tricks and told them all his jokes, something he never did in the previous rounds. He was in a good space and knew what to expect.
Mason’s last chemo in May 2014.
On May 21, 10 days before his seventh birthday, he had his broviac line removed. Forty eight hours later, he was able to lay down in a bath for the first time in months. He lay in that tub until the water went cold. I will never forget the look on his face that day. There was so much peace.
We have spent our days since then trying to find our new normal, finding joy in every day. Although that year was the worst year ever for us, we really are the lucky ones. Our family is whole and we count our blessings every day for that.
One of our normals includes being part of the Kids Cancer Care Foundation of Alberta, an organization we are so lucky to be part of. They include us in so many amazing activities and events, but the very best one of them all is Camp Kindle. This past summer our boys were able to go to camp again. Bennett and Mason LOVE camp. They meet kids who know exactly what life with, during, and after cancer is like. They meet lots of kids and quickly make life-long friends. They swim, hike, sing, laugh and have genuine fun.
Diego and I have also been to Camp Kindle ourselves, once for Family Camp and once for Survivor Day. What a magical place. The peaceful environment overtakes any stress or outside noise in your head. If you ever get a chance to visit, go. You’ll know exactly what I’m talking about.
Mason and Bennett love going to Camp Kindle.
Kids Cancer Care isn’t just about the delicious pizza they deliver every Wednesday on the unit at the hospital and camp though. This incredible organization has done so much for our family. They filled our freezer with delicious food when Mason was in treatment. They include families in so many awesome Kids Cancer Care events — theatre tickets, sporting events, going to the North Pole on the Polar Express, galas, even golf tournaments.
Meeting other families who have experienced a lot of what we have gone through is also something we truly cherish. We have become part of this incredible family none of us really wanted to join, but we all feel so lucky to be part of. Kids Cancer Care also always include siblings, which is so very important because brothers and sisters go through the horrors of the cancer journey too. They witness many things kids shouldn’t see. Bennett was with his little brother every step of the way, holding his hand and encouraging him every day. Bennett was Mason’s biggest fan. Mason is lucky to have such an amazing big brother.
Mason and Dad Diego on The Polar Express with Kids Cancer Care.
Another reason we love Kids Cancer Care so much is that they continue to keep us part of the programs and activities even after treatment is over. They know that even when chemotherapy, radiation or transplants are done, our journey along the medical path is far from over.
Hopefully there will be a day in the near future when pediatric cancer is extinct, but until then, organizations like Kids Cancer Care need your support to help families like ours to find peace, joy and love again during and after the horrific diagnosis of childhood cancer. We truly don’t know where we would be without their incredible support system.
We will never be able to thank Kids Cancer Care enough, or be able to express how much gratitude we have for Kids Cancer Care. Thank you Kids Cancer Care for all you do for us and all of the families you take care of.
~Jennifer Rodriguez, Mason’s Mom
“It has been amazing to be recognized nationally for this research but more important, is knowing that the research may actually have potential in the real world.” ~ Colette Benko
Colette Benko isn’t your average 15-year-old. Not because she’s already conquered cancer once, but because of her scientific mind and insatiable curiosity. If Colette has it her way, she’ll be conquering cancer the rest of her life, but this time, it will be from the inside of a research lab.
Thanks to you, Colette was able to start feeding her curiosity while working as a summer research student in Dr. Aru Narendran’s laboratory at the University of Calgary. But this wasn’t the first time Colette had been in a research lab.
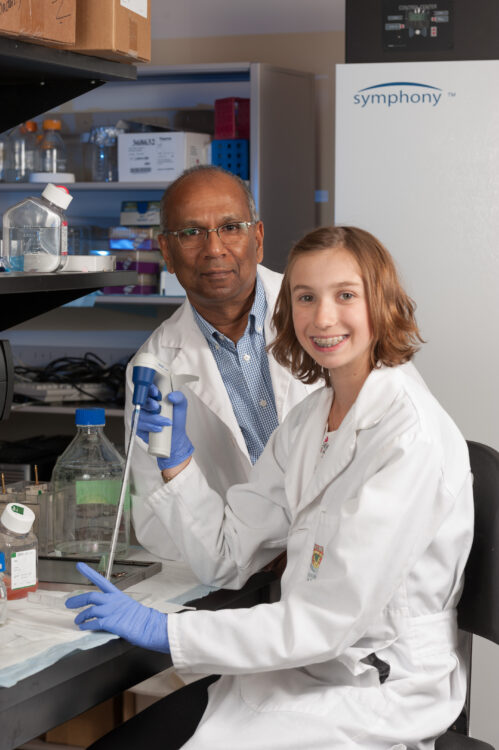
Colette Benko is enjoying a productive mentorship with University of Calgary researcher Dr. Aru Narendran.
For the past two years, Colette has been enjoying a rewarding and successful mentorship with Dr. Narendran, a pediatric oncologist at the Alberta Children’s Hospital and an Experimental and Applied Therapeutics (ExpAT) researcher in the Childhood Cancer Research Program at the University of Calgary.
Colette first met Dr. Narendran at the Alberta Children’s Hospital when she was being treated for synovial sarcoma, a cancer of the joints and soft tissue.
“I’ve always been a science nerd, but I had never done a medical science research project,” says Colette. “When Dr. Narendran found out that I love science so much, he agreed to mentor me. He’s been a great mentor. He’s so kind and patient and he’s so committed.”
“When Colette talked to me about wanting to do research in our laboratory I was impressed by her extraordinary self-assurance, energy and keenness,” says Dr. Narendran. “She reminded me of that Ivern Ball quote, ‘Knowledge is power, but enthusiasm pulls the switch.’”
The outcome of that enthusiasm has been two award-winning research projects for Colette.
Last spring, she won a silver medal for excellence in the 2016 Canada-Wide Youth Science Fair and a $2,000 scholarship for her research into a potential new therapy for neuroblastoma, a cancer of the sympathetic nervous system often found in infants and young children. In 2014, her research into an extremely rare and aggressive brain cancer in infants called ATRT won gold in the Calgary Youth Science Fair.
“It’s so incredible to work in a lab,” she says. “To actually experience and see results, not just read about it, is so satisfying.”
Colette is especially excited about the results of the neuroblastoma research, because it may actually have practical application in the world of pediatric cancer one day.
“It has been amazing to be recognized nationally for this research, but more important, is knowing that the research may actually have potential in the real world,” Colette says.
Working with students in Dr. Narendran’s lab, Colette was studying a unique new drug against three types of neuroblastoma and found that it inhibited growth in all three by stopping the action of a protein called EZH2, which is involved in blocking tumour suppressor genes.
“Normally, our cells rely on a group of molecules called tumour suppressor genes, which constantly act to prevent malignant changes in cells, by causing them to self-destruct,” she says. “But some tumour cells overproduce a protein that actually turns off tumour suppressor molecules, so the cancer cells continue to grow. The drugs we’re studying, known as the EZH2 inhibitors, aim to block this abnormal mechanism in neuroblastoma cells.”
When Colette presented her findings at the 2016 Canada-Wide Youth Science Fair, researchers investigating similar ideas were excited to see her data, as this drug has also shown effectiveness against pediatric brain tumours.
Still in the early stages, Colette’s findings seem to suggest that the drug may not only be inhibiting cancer growth; they may actually be inducing cellular death in the neuroblastoma cells. Another promising attribute of the drug is it doesn’t seem to attack regular cells, which could mean fewer side-effects for patients.
Working as a summer research student in Dr. Narendran’s lab this year, Colette was able learn more about the necessary processes involved in conducting cancer research, while also developing her understanding of the biology of various pediatric cancers.
Colette also continued generating data on her neuroblastoma project, testing whether the drugs are actually capable of inducing death in neuroblastoma cells and assessing what effect, if any, they may have on non-cancerous cells.
After graduating from high school, Colette plans to take her quest for a cure even further. She plans to pursue a Bachelor of Health Sciences at the University of Calgary and follow that with post-graduate work in pediatric cancer research.
Thank you for making our summer student research program possible. While providing scientists with much-needed help in the lab, the program helps ensure that promising young research talent is nurtured for tomorrow.
Drs. Vanessa Meier-Stephenson(L) and Dr. Aru Narendran (R) have been mentoring Colette Benko, a summer research student, in their University of Calgary laboratory.
On September 15, 2016, the Pediatric Oncology Experimental Therapeutics Investigators Consortium (POETIC) and CorMedix Inc., announced a powerful new partnership in the fight against childhood cancer. With the new partnership agreement, POETIC and CorMedix will work together to develop a promising drug called CRMD-005 as a potential treatment for rare children’s tumours, including neuroblastoma and osteosarcoma.
CRMD-005 is a proprietary form of Taurolidine, an anti-microbial currently used to prevent infections in catheters. A safe product that causes very few side-effects, Taurolidine is also being studied as a treatment for cancer.
The new research effort will begin with pre-clinical studies to demonstrating its role in immunotherapy on pediatric cancer models in the laboratory. Laboratory studies show that Taurolidine is capable of inhibiting the growth of cancer cells at concentrations of 100 times lower that that which is needed for the drug’s antibiotic activity, suggesting the drug’s high tolerability (the degree to which overt adverse effects of a drug can be tolerated by a patient).
Working with POETIC physicians and scientists, Dr. Aru Narendran will lead the pre-clinical efforts, which will involve further defining Taurolidine’s potential role in treating pediatric cancers, especially in relapsed and drug-resistant cancers. It will also involve identifying the best drugs to combine with Taurolidine to plan for and test in future clinical trials.
Dr. Aru Narendran will lead the pre-clinical research effort to better understand the effect of Taurolidine on pediatric cancer.
“Our goals are to better elucidate Taurolidine’s mechanism effects and leverage its history of safety to maximize its anti-neoplastic potential in an intelligent and efficient manner,” said Dr. Narendran, a Kids Cancer Care-funded researcher in the Experimental and Applied Therapeutics Research effort at the Children’s Cancer Research Program at the Alberta Children’s Hospital and University of Calgary.
The program will involve collaboration with several National Cancer Institute centers that are part of the POETIC group, including Memorial Sloan Kettering Cancer Center (MSK), Weill Cornell Medical Center, Alberta Children’s Hospital, and other top tier cancer centers of excellence.
POETIC is a network of pediatric oncologists and researchers from 10 top-tier academic medical research centers, who are collaborating across institutions to bring promising new therapies into phase one and phase two clinical trials for children with cancer.
CorMedix is a bio-pharmaceutical company that develops and brings to market therapeutic agents to prevent and treat infectious and inflammatory disease.
POETIC recognizes Kids Cancer Care with Partner of Distinction Award
POETIC recently recognized Kids Cancer Care’s contribution to childhood cancer research with a prestigious POETIC Partner of Distinction Award. The award recognizes our ongoing support of Dr. Aru Narendran and his research team at the Alberta Children’s Hospital Research Institute and the University of Calgary. Dr. Narendran is an Experimental and Applied Therapeutics researcher at the Childhood Cancer Research Program. The only Canadian member of POETIC, Dr. Narendran is currently the lead investigator in three phase one POETIC clinical trials.
Children with cancer experience pain, often severe and prolonged, over the course of their disease and treatment. The Cancer Knowledge Network (CKN) is partnering with The Centre for Pediatric Pain Research and a research team of internationally known health researchers and clinicians led by Dr. Christine Chambers (IWK Health Centre) and Dr. Jennifer Stinson (SickKids) to bring the best research evidence about children’s cancer pain to parents through social media.
Unfortunately, we know that children with cancer don’t always receive the best pain management possible and that parents are often looking for more solutions at a time when they are stressed and exhausted. We cannot think of a better way to use our trusted CKN platform than to fast track evidence-based information to parents, empowering them to serve as powerful advocates to help improve their children’s pain management.
With a research grant from the Canadian Cancer Society, the Cancer Knowledge Network and The Centre for Pediatric Pain Research are addressing this problem through a social media campaign designed especially for parents, called Making Cancer Less Painful For Kids (#KidsCancerPain).
Over the next 12 months, they will be bringing parents the very best, cutting-edge research evidence about children’s cancer pain – what causes it, how to assess it, how to treat it, common myths, and more! They’ll be sharing this information with parents through a series of blogs, videos, images, Facebook posts, and Twitter chats, all posted and shared on the Cancer Knowledge Network’s website and social media. The research team will be studying the reach of the campaign and its impact on parents.
Having battled leukemia twice, Gordon Brooke understands the importance of developing and testing new drugs that will save kids’ lives without causing permanent side effects.
The first time he was diagnosed with acute lymphoblastic leukemia (ALL), Gordon underwent punishing amounts of chemotherapy and a steroid dose so strong it hindered his ability to walk.
“I was bald, ghost pale, skeletal and almost entirely anti-social,” he says.
While on treatment, Gordon received high doses of chemo and a steroid dose so high it hampered his ability to walk.
When he relapsed three years later, Gordon’s only hope for survival was a bone marrow transplant (BMT). A BMT is a grueling procedure, in which the patient’s white blood cells are wiped out by high-dose chemotherapy and replaced by a donor’s healthy new blood cells.
The transplant saved Gordon’s life.
When Gordon relapsed, his only hope for survival was a bone marrow transplant.
Although BMTs frequently cures cancers and other disorders of blood is the treatment, it is a brutal procedure and the risk of developing complications is high. Roughly 25 to 40 per cent of adult and pediatric BMT patients develop a condition called graft versus host disease (GvHD), which occurs when donor-derived blood cells in a patient see the patient’s body as foreign and triggers an immune response, leading to serious health problems and complications. About 10 per cent of these patients die from GvHD.
Developing new drugs for young people with high-risk cancers is vital and, one day, Carfilzomib may be one of those drugs.
Carfilzomib is currently being evaluated in a phase I clinical trial for difficult-to-treat pediatric cancers at 10 top-tier pediatric hospitals across North America. Open to all eligible children with relapsed leukemia and solid tumours, the study will closely monitor and analyze the side effects of Carfilzomib to determine the maximum dose children can safely tolerate. The trial will cost approximately $3.5 million (U.S.) to administer and is being run through the Pediatric Oncology Experimental Therapeutics International Consortium (POETIC).
Dr. Aru Narendran is the lead investigator in the phase I clinical trial testing the effects of Carfilzomib on children with high-risk cancers.
Previously tested and approved for use in adults, Carfilzomib is already showing promise for treating adult patients with multiple myeloma — a high-risk leukemia. Studies on Carfilzomib in a University of Calgary lab revealed a similar penchant for killing pediatric cancer cells. These findings from Dr. Narendran’s lab were presented last year at the American Association of Cancer Research.
Dr. Narendran and Dr. Jessica Boklan of Phoenix Children’s Hospital are the principal investigators in the clinical trial and Dr. Tony Truong, co-principal investigator at the Alberta Children’s Hospital, and U of C clinical research staff Karen Mazil and Pina Giuliano, are helping monitor side effects and analyze findings from the study.
Carfilzomib is a proteasome inhibitor, meaning it stops the proteasome mechanism in cancer cells that helps cancer to survive. Because cancer cells divide and multiply so quickly they make a lot of mistakes, leading to abnormally formed cells. These poorly formed cells put stress on the cancer and threaten its survival. To get around this, the cancer cell uses proteasomes to repair its mistakes. By inhibiting the proteasome, Carfilzomib helps the cancer kill itself by its own imperfections.
“The beauty of this drug is it’s not cancer-specific,” says Dr. Narendran a pediatric cancer researcher with the Experimental and Applied Therapeutics (ExpAT) program at the Childhood Cancer Research Program at the Alberta Children’s Hospital Research Institute and the University of Calgary. “It blocks a mechanism that is vital to pretty much all malignant cells, so it can be used against different cancers. Normal cells don’t make so many mistakes, so this drug will be less toxic to normal cells, which may mean fewer side effects for children.”
Another promising attribute of Carfilzomib is that it works synergistically with other chemotherapies to boost their ability to kill cancer cells. This is especially important for chemo-resistant cancers.
“It’s kind of a safety net,” says Dr. Narendran. “Because the chemo agents and their toxicity are already known to us, we can use these chemotherapies with Carfilzomib to boost their potency for better outcomes.”
“What we know so far comes only from adult patients or from laboratory studies against pediatric cancer cells,” says Dr. Narendran. “We do not know if it will actually offer any benefit to pediatric cancer patients yet.”
As a phase I clinical trial, the study is not intended to cure children, but to understand its toxicities and determine suitable doses for treating children in the future.
Still, it is the first important step in a long quest to find safe and effective treatments for children with incurable cancers. If it lives up to its potential, Carfilzomib may one day offer hope for children with high-risk cancers.
Gordon with his mother Lauren Warwick. With the help of a Kids Cancer Care scholarship, Gordon is studying pharmacology.
Fortunately, Gordon Brooke has not experienced complications from the BMT he received. He’s healthy and strong today and with the help of a Kids Cancer Care scholarship Gordon is studying pharmacology at the University of Alberta. His experiences with cancer and chemotherapy inspired him to pursue a career in pharmacological research. One day, Gordon hopes to use his expertise to further refine chemotherapies to help young people like him.
Thank you to our generous fundraising partners who make our programs and services possible























 CRMD-005 is a proprietary form of Taurolidine, an anti-microbial currently used to prevent infections in catheters. A safe product that causes very few side-effects, Taurolidine is also being studied as a treatment for cancer.
CRMD-005 is a proprietary form of Taurolidine, an anti-microbial currently used to prevent infections in catheters. A safe product that causes very few side-effects, Taurolidine is also being studied as a treatment for cancer.